Using dataflow diagrams to support research informed consent data management communications: participant perspectives
Brian J McInnis, Ramona Pindus, Daniah H Kareem, Julie Cakici, Daniela G Vital, Eric Hekler, Camille Nebeker
Journal of the American Medical Informatics Association, 4 February 2025
Abstract
Objectives
Digital health research involves collecting vast amounts of personal health data, making data management practices complex and challenging to convey during informed consent.
Materials and Methods
We conducted eight semi-structured focus groups to explore whether dataflow diagrams (DFD) can complement informed consent and improve participants’ understanding of data management and associated risks (N = 34 participants).
Results
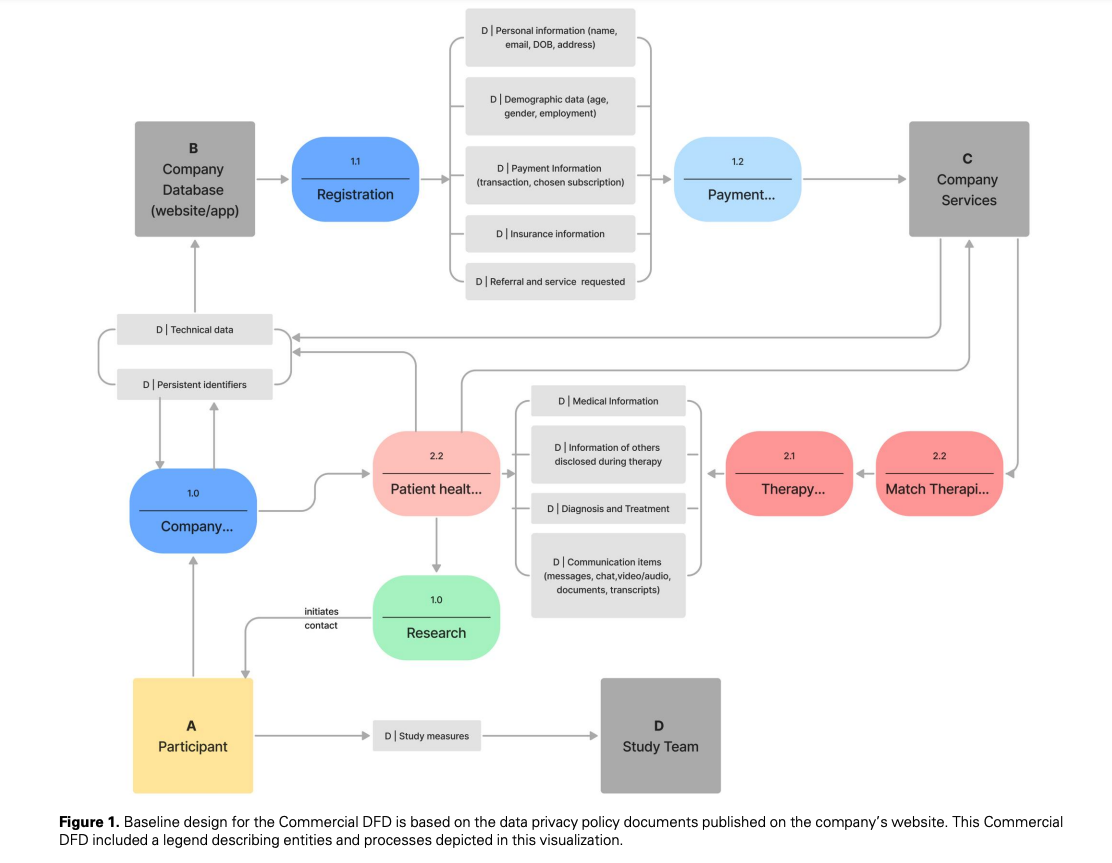
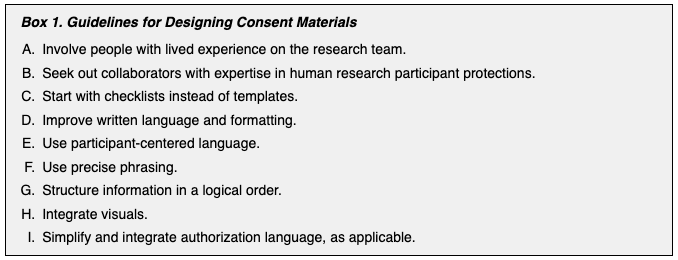
Our analysis found that DFDs could supplement text-based information about data management and sharing practices, such as by helping raise new questions that prompt conversation between prospective participants and members of a research team. Participants in the study emphasized the need for clear, simple, and accessible diagrams that are participant centered. Third-party access to data and sharing of sensitive health data were identified as high-risk areas requiring thorough explanation. Participants generally agreed that the design process should be led by the research team, but it should incorporate many diverse perspectives to ensure the diagram was meaningful to potential participants who are likely unfamiliar with data management. Nearly all participants rejected the idea that artificial intelligence could identify risks during the design process, but most were comfortable with it being used as a tool to format and simplify the diagram. In short, DFDs may complement standard text-based informed consent documents, but they are not a replacement.
Discussion
Prospective research participants value diverse ways of learning about study risks and benefits. Our study highlights the value of incorporating information visualizations, such as DFDs, into the informed consent procedures to participate in research.
Conclusion
Future research should explore other ways of visualizing consent information in ways that help people to overcome digital and data literacy barriers to participating in research. However, creating a DFD requires significant time and effort from research teams. To alleviate these costs, research sponsors can support the creation of shared infrastructure, communities of practice, and incentivize researchers to develop better consent procedures.