Giving Due Weight to Children and Young People in Australian Policy Making
Meaghan Vosz, Anne Graham, Mark Hughes
The International Journal of Children’s Rights, 17 December 2024
Abstract
While Article 12 of the Convention on the Rights of the Child is often cited to assure children’s right to express their views freely in all matters affecting them, little is known about the practices associated with giving due weight to their views in policy-making that impacts their lives. This paper reports on critical-participatory research exploring the practices of more than 100 policy actors, conducted with five young co-researchers with lived experience of Australian child protection and out-of-home care systems. Practices associated with giving due weight included: involving children as policy actors, listening, giving feedback and reporting back, and amplifying their views. Practices were constrained by discourses of authenticity/tokenism; bureaucracy and jurisdiction; the attribution of expertise; and limited funding and time. Research demonstrated opportunities for realising Article 12 through intergenerational dialogue and valuing the lived experience and agency of young people as policy actors.
A New Approach for Investigating Children’s Participation Rights in Early Childhood Education: Listening to Voices in Interaction for Participation (LViIP)
A New Approach for Investigating Children’s Participation Rights in Early Childhood Education: Listening to Voices in Interaction for Participation (LViIP)
Cynthia Hicban, Maryanne Theobald, Julia Mascadri
The International Journal of Children’s Rights, 17 December 2024
Abstract
Research into children’s participation rights has largely focused on the challenges for early childhood educators to navigate children’s participation rights enactment. The aim of this article is to show how the enactments of children’s participation rights in an educational setting can be identified using a new approach, Listening to Voices in Interaction for Participation (LViIP).
LViIP is based on Lundy’s (2007) conceptualisation of Article 12(1) and combines with conversation analysis (ca) to identify how rights enactment sequentially unfolds and how the interactants mobilise (or gatekeep) opportunities for children to have a say.
A step-by-step worked example of LViIP shows in detail how participatory approaches by educators and children are built in early childhood education, thus demonstrating which interactional practices contribute towards the co-construction of children’s participation rights and how early childhood professionals can listen, be and do as duty-bearers of children’s rights in their daily practice.
Guidelines for the Creation of Accessible Consent Materials and Procedures: Lessons from Research with Autistic People and People with Intellectual Disability
Guidelines for the Creation of Accessible Consent Materials and Procedures: Lessons from Research with Autistic People and People with Intellectual Disability
Research Article
Kelly B. Beck, Kristen T. MacKenziem, Anne V. Kirby, Katherine McDonald, Ian Moura, Kaitlyn Breitenfeldt, Elizabeth Rutenberg, Tanvi Kumar, Juliet Mancino, Maya Sabatello, Shannon Roth, Christina Nicolaidis
Autism in Adulthood, 19 February 2025
Abstract
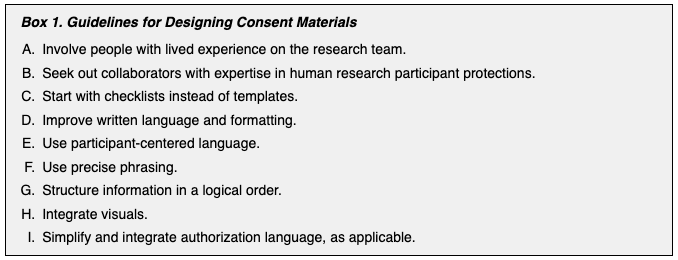
Informed, voluntary, ongoing consent is a central tenet of ethical research. However, consent processes are prone to exclusionary practices and inaccessibility. Consent materials are often too long and complex to foster understanding and ensure that people make truly informed decisions to participate in research. While this complexity is problematic for all people, these challenges are compounded for autistic people and people with intellectual disability. Consent materials and procedures rarely incorporate accommodations for processing and communication differences common in autism and intellectual disability. Failure to provide such accommodations ultimately threatens the conduct of ethical research. We describe lessons learned across multiple major U.S. research institutions that improved informed consent materials and procedures, with the goal of fostering responsible inclusion in research for autistic people and people with intellectual disability. We used these alternative materials and procedures in multiple research projects with samples of autistic people and people with intellectual disability. Each contributing team partnered with university human research participant protections personnel, accessibility experts, community members, and researchers to develop rigorous procedures for improving the readability and accessibility of informed consent materials. We present guidelines for designing consent materials and procedures and assert that participatory methods are vital to the success of ongoing accessibility initiatives. Adoption of understandable consent materials and accessible consent procedures can cultivate more equitable, respectful, and inclusive human research practices. Future work should expand on this work to design inclusive practices for populations with additional considerations.
Consent Mechanisms and Default Effects in Health Information Exchange in Japan
Consent Mechanisms and Default Effects in Health Information Exchange in Japan
Original Research
Atsushi Ito, Fumihiko Nakamura
Frontiers in Digital Health, 3 February 2025
Background
Health information exchange (HIE) is an information system that efficiently shares patient information across medical institutions. However, traditional consent methods, represented by opt-in and opt-out, face a trade-off between efficiency and ethical, making it difficult to fundamentally improve consent rates. To address this issue, we focused on default settings and proposed an innovative approach called the “two-step consent model,” which leverages the advantages of existing models using utility theory. We evaluated the acceptability of this method.
Methods
An online survey was conducted with 2,000 participants registered with Japan’s largest internet survey company. We compared and analyzed the consent rates of the opt-in, opt-out, and two-step consent models. Results: The opt-in model had a 29.5% consent rate, maximizing patient autonomy but increasing the burden and reducing efficiency. The opt-out model had a 95.0% consent rate but raised concerns among half of the respondents. The two-step consent model had a 68.5% consent rate, demonstrating its cost-effectiveness compared with traditional models
Discussion
The two-step consent model, involving implicit and explicit consent when needed, ensures efficient consent acquisition while respecting patient autonomy. It is a cost-effective policy option that can overcome the ethical issues associated with the opt-out model. Introducing methods that leverage both opt-in and opt-out advantages is expected to address HIE stagnation.
Conclusion
The two-step consent model is expected to improve consent rates by balancing the efficiency and quality of consent acquisition. To achieve this, patient education is crucial for raising awareness and understanding of HIE and its consent methods.
Surgical informed consent practice and associated factors among adult postoperative patients in public hospitals of Mekelle, Tigray, Ethiopia 2023/2024
Surgical informed consent practice and associated factors among adult postoperative patients in public hospitals of Mekelle, Tigray, Ethiopia 2023/2024
Research Article
Fiseha Abadi Gebreanenia, Hailemarim Berhe Kahsay, Desta Siyoum Belay, Binyam Gebrehiwet Tesfay, Fissha Brhane Mesele, Mamush Gidey Abirha
PLOS One, 3 February 2025
Open Access
Abstract
Background
Substantial weaknesses and omissions of surgical informed consent are evident and the current elements of the surgical informed consent process are largely neglected in daily practice. This study aimed to assess surgical informed consent practice and associated factors among adult postoperative patients in public hospitals of Mekelle, Tigray, Ethiopia.
Methods
Institution based cross-sectional study was conducted among 314 adult postoperative patients in public hospitals of Mekelle, Tigray, Ethiopia. Participants were selected using systematic random sampling. A pretested interviewer-administered questionnaire was used to collect data. Descriptive, Descriptive, bivariate and multivariable logistic regression analyses were performed using statistical package for social science version 27.
Result
Only 35.8% (CI 95%, 30.6, 41) of the respondents were identified to have received the recommended (6 or more) components of surgical informed consent. Educational level [AOR 5.76 (1.02, 32.6)], timing of surgical informed consent delivery [AOR 3.27 (1.5, 7.11)], qualification of counselor who took surgical informed consent them [AOR3.185 (1.21, 8.38)], hospital type [AOR 2.85 (1.26, 6.46)], and duration of counseling [AOR 6.9 (3.33, 14.3)] were statistically significant at P<0.05.
Conclusion
Majority of participants did not receive comprehensive information during the surgical informed consent process in the study hospitals. To improve the delivery it is suggested that health professionals; create rapport with patient, spend more time during counseling.
A Critical Appraisal of Informed Consent in English Medical Law: A Patient-Centred Approach Against Medical Paternalism: Who Gets to Decide What Is Best for Me?
A Critical Appraisal of Informed Consent in English Medical Law: A Patient-Centred Approach Against Medical Paternalism: Who Gets to Decide What Is Best for Me?
Lisa Kachina Poku
European Journal of Health Law, 18 February 2025
Abstract
This article seeks to discuss informed consent in English law. The attitudes on informed consent have shifted to a more patient-centred approach following Montgomery v Lanarkshire Health Board [2015] UKSC 11, [2015] AC 1430, as opposed to the long-standing Bolam decision where clinical judgment was more widely accepted. Thus, following on from the decision in Montgomery a patient is required to know about material risks regarding the proposed treatment and not what the doctor thinks would be the best practice as has been the long-standing consensus since Bolam was decided back in 1957 with subsequent cases following suit. The Montgomery principle has allowed more transparency in the patient–doctor relationship, allowing for a discussion between the doctor and the patient to be the central focus. The outcome of Montgomery was a much needed change in healthcare because prior to this it could be seen that patients were having decisions made on their behalf, and if they had been informed accordingly regarding the risks involved may have decided not to go ahead with the procedure. In the case of Diamond v Royal Devon & Exeter NHS Foundation Trust [2019] EWCA Civ 585 the case highlights the issue of causation in medical negligence action if a doctor does not warn of risks and advise treatment alternatives this would not result in a claim for damages because the patient in this case as was held would have gone ahead with the mesh repair in any case, and thus failing to establish causation could result in no remedy as it did in Diamond. Furthermore, the recent case of McCulloch and others v Forth Valley Health Board [2023] UKSC 26 adds a bit of salt to the wounds of those who had thought or believed that Montgomery had already clarified the position regarding disclosure of alternative treatments to a patient, and to our dismay to learn of that once again English courts have ruled in favour of ‘Bolam’.
Informed consent in neurosurgery with particular reference to alternatives to proposed surgery. Updated case law including McCulloch.
Informed consent in neurosurgery with particular reference to alternatives to proposed surgery. Updated case law including McCulloch.
Research Article
Nicholas Todd, James Wright-Todd
Medico-Legal Journal, 11 February 2025
Abstract
Introduction
Informed consent is a crucial element in neurosurgical practice; failures of the consenting process are a common cause of litigation in neurosurgery and judgments that have particular relevance to neurosurgical practice will be reviewed here. Guidance for consent based upon current case law is discussed.
Methods
The legal databases BAILII and WestLaw were searched using the search term “informed consent”. The BAILII search yielded 86 abstracts, WestLaw yielded 33. There were 15 duplicates. Ten of the remaining 104 abstracts were commentaries, leaving 94 judgments. From those judgments a further 21 cases were added. A total of 115 judgments were reviewed by both authors.
Results
A total of 23 judgments dealing with issues of informed consent in neurosurgical and other surgical practice were selected. The cases and their implications for neurosurgical consent are discussed below.
Discussion
When proposing a surgical procedure to a competent adult, the treating surgeon must discuss the benefits, risks and alternatives to treatment with the patient. The surgeon can be guided by professional guidance from the GMC, or another professional body, and/or case law. Relevant issues include: (i) the risks and benefits of surgery; (ii) information that is accurate (or inaccurate, incorrect, missing or late information); (iii) established practice; (iv) the current state of knowledge; (v) reasonable alternative treatments; and (vi) surgery performed on a different day or by a different surgeon.
Perceptions and experiences of healthcare professionals of implementing the Organ Donation (Deemed Consent) Act in England during the Covid-19 pandemic
Perceptions and experiences of healthcare professionals of implementing the Organ Donation (Deemed Consent) Act in England during the Covid-19 pandemic
Research
Mustafa Al-Haboubi, Leah McLaughlin, Lorraine Williams, Jane Noyes, Stephen O’Neill, Paul Boadu, Jennifer Bostock, Nicholas Mays
BMC Health Services Research, 31 January 2025
Open Access
Abstract
Context
In May 2020 during the COVID-19 pandemic, England implemented a ‘soft’ opt-out system of consent to deceased organ donation. As part of a wider evaluation, this analysis focused on the perceptions of health care professionals, specifically their experiences of implementation.
Methods
Mixed-methods study informed by Normalisation Process Theory, based on two national surveys of health care professionals and interviews, observations and document analysis, across two case study sites. Routine NHS Blood and Transplant’s audit data provided context.
Findings
70 interviews with 59 staff and 244 first and 738 second surveys. COVID-19 affected every aspect of implementation. Although supportive in principle, many staff were unconvinced that legislative changes alone would increase consent rates. Many staff were redeployed or left their jobs. As a result, staff were not able to work collectively as intended for implementation. Staff received routine donor audit data suggesting the law was yet to make a difference to consent rates, reducing their enthusiasm and commitment.
Conclusions
Implementation could have been more impactful if delayed. The National Health Service needs to reprioritise organ donation and relaunch the implementation plan in the post-pandemic period, though it is unlikely the changes will bring about a significant increase in consent rates.
Role and Complexities of Informed Consent in Vascular Surgery
Role and Complexities of Informed Consent in Vascular Surgery
Editorial
Himanshu Verma
Indian Journal of Vascular and Endovascular Surgery, January – March 2025; 12(1)
Open Access
Introduction
Informed consent is a cornerstone of ethical medical practice, emphasizing the patient’s right to autonomy and the alignment of medical care with their values and preferences. Over the past century, this principle has evolved from a procedural formality to an essential process enabling shared decision-making (SDM). Patients now actively participate in treatment decisions, weighing the risks, benefits, and alternatives of interventions to ensure their choices reflect personal goals and priorities.
While patient comprehension remains a critical element of informed consent, studies reveal significant gaps in understanding.[4] Patients often struggle to recall or fully grasp essential details, including diagnoses, procedural risks, benefits, and alternatives.[5,6] Consequently, informed consent has transitioned from being a mere legal safeguard to an interactive dialog fostering patient engagement and trust.[7,8] This editorial explores the nuances of informed consent, particularly within the context of vascular surgery, where challenges are multifaceted and deeply rooted in both medical complexity and patient perception.
Broad consent in the emergency department: a cross sectional study
Broad consent in the emergency department: a cross sectional study
Research
Antje Fischer-Rosinský, Larissa Eienbröker, Martin Möckel, Frank Hanses, Felix Patricius Hans, Sebastian Wolfrum, Johannes Drepper, Philipp Heinrich, Anna Slagman
Archives of Public Health volume, 18 February 2025
Open access
Abstract
Background
The Medical Informatics Initiative (MII) introduced a broad consent form (MII-BC) encompassing clinical, insurance, and biomaterial data, along with re-contacting options. In the emergency department (ED), outpatient and inpatient patients of all illnesses and severity could be reached early in their treatment course. The BC-ED (Broad Consent in the Emergency Department) project uniquely investigated the implementation of MII-BC in EDs, exploring feasibility, selection bias and patients’ perceptions of voluntariness, information recall, motivation, and satisfaction.
Methods
The BC-ED project involving four university hospital EDs in Germany, is part of CODEX+ (Collaborative Data Exchange and Usage), an initiative within the Network University Medicine (NUM). To minimize selection bias, a systematic sampling approach (every 5th/30th patient) was applied, with patient recruitment and consent processes adapted to local conditions and therefore varying among sites. Data collection included patient questionnaires, surveys completed by study nurses, and routine clinical data. Analysis was conducted descriptively using SPSS.
Results
Of 1,138 patients approached, 553 (48.6%) were capable of giving consent. Of 353 patients who could not consent, primary reasons included language barriers (35.4%) and inability to grasp study details (21.5%). Of all eligible patients, 3.3% could not be contacted. Of 535 (47.0%) patients able to consent and contacted, 313 consented to the MII-BC. Resulting in a consent rate of 27.5% corresponding to the baseline population and 58.5% of those contacted. Motivations for consenting were general support for research (85.3%) and the desire to help future patients (78.2%). Patients generally reported a high level of understanding and satisfaction with the consent process, reporting comprehensive understanding of scientific data use (89.8%) and associated risks (82.2%). However, discrepancies were noted between consented options and patient recall.
Conclusions
This study is the first to investigate the implementation of the MII-BC in the challenging ED environment. With a consent rate of 27.5% total baseline population and 58.5% of those contacted, it demonstrates that patients were able and willing to participate in research. Reasons for non-consent were barriers like language and medical conditions. Strategies to address these barriers are crucial for inclusivity. Although patients generally understood the consent process, discrepancies in recall highlight the need for improved comprehension strategies.
